

Cell-free DNA (cfDNA) extracted from peripheral blood plasma has been increasingly used as a non-invasive approach for diagnosis and surveillance of solid and hematologic malignancies. Somatic variants associated with clonal hematopoiesis of indeterminate potential (CHIP) are commonly detected in such liquid biopsies, suggesting that cfDNA may be useful for their detection. CHIP has emerged as a predictor of progression to hematological malignancies; however, clones are still largely detected using peripheral blood (PB) and bone marrow (BM) cells.
In this study, we investigated the performance of cfDNA for detection and quantification of CHIP compared to matched PB/BM cells. cfDNA initially was collected from a healthy cohort (n=106), part of the Baltimore Longitudinal Study of Aging/NIH; later we expanded to screen patients with aplastic anemia (AA; n=53) and myelodysplastic syndrome (MDS; n=27) monitored at the National Heart, Lung, and Blood Institute. Samples were screened for somatic mutations in myeloid neoplasm-related genes using a commercial panel of 177 genes.
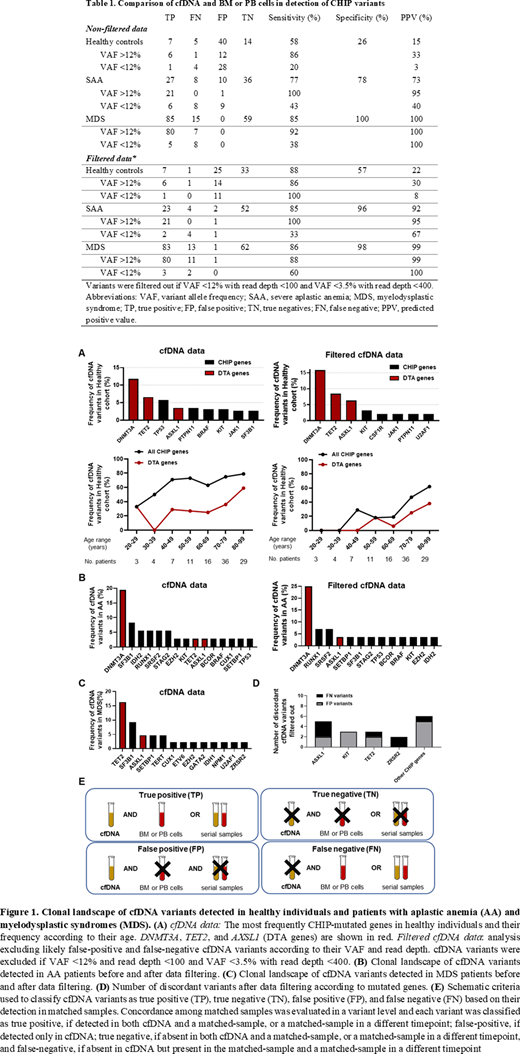
In HC (median age:72 [range:24-96]), 78/106 subjects (73%) were found to have one (28%) or two and more (45%) cfDNA variants in CHIP-related genes, most frequently in DNMT3A,TET2, TP53, and ASXL1 (Figure 1A). CHIP was observed in more than 60% of individuals older than 40 years, higher than typically reported. In contrast, only 17/53 of AA patients (32%; median age:51 [range:13-82]) were found to have one (n=10) or two or more (n=7) cfDNA variants, most commonly DNMT3A and SF3B1 (Figure 1B). In MDS, 17/29 (58%; median age:63 [range:35-85]) had one (n=10) or two or more (n=7) variants, TET2 and SF3B1 being most frequent (Figure 1C). Median VAF of cfDNA variants was significantly different among cohorts (HC:2.5% [95CI%:2-4] vs AA:18% [95CI%:6-32] vs MDS:38.6% [95CI%:27-42]; t-test,p<000.1).
cfDNA results were validated against matched PB/BM cells collected from HC (n=25), AA (n=56), and MDS patients (n=54). cfDNA variants were classified as true, and false positives or negatives according to their presence in PB/BM (Figure 1E). In HC, cfDNA sensitivity was moderate (58%), but specificity and PPV were low compared to PB. In AA and MDS, sensitivity, specificity and PPV values were high compared with BM (Table 1). In all cohorts, the median VAF of discordant variants was significantly lower than VAF of true-positives (9.5% [95CI%:8-12] vs. 36% [95CI%:31-37]; t-test,p<000.1). Discordant pairs were mainly observed with cfDNA variants at VAF<12%; the sensitivity and PPV of variants below this threshold were very low (Table 1). Variants' discordance was correlated with sequencing coverage. Median read depth of false-positives and false-negatives was 112 (95CI%:92-143) compared to 464 [95CI%:355-563]) in true-positives. By filtering out likely discordant cfDNA variants using VAF and read depth, concordance significantly improved (Table 1). In HC, DTA genes were most commonly mutated (while TP53 variants were filtered out) and CHIP frequency was lower than in previous analysis (30% vs 60% in HC at >40yo; Figure 1A). Discordant pairs were found most often in ASXL1, KIT, TET2, and ZRSR2 (Figure 1E). Although linear regression showed high correlation between the VAF of paired samples (R2>0.7), agreement of VAF by Bland-Altman analysis was poor; this approach calculates the bias, the mean difference between the VAF of matched samples, and its standard deviation (SD) to more accurately evaluate agreement between paired values. Here, the bias and SD were both as high as 9% in HC and patients. These large variations translated to a wide range of upper and lower limits of agreement (mean ± 2*SD), which represent the limits of acceptable differences.
In summary, the landscape of somatic cfDNA variants depended on variant VAF. Technical factors were an important source of assay discordance, and although cfDNA variants were reliably detected at higher VAFs, their quantification was not comparable to VAF detected in blood cells. A single cfDNA clone varied up to 9% in size and SD was unacceptably high in all cohorts. cfDNA and PB/BM may not be interchangeable, as cfDNA may either over- or under-estimate clone size, regardless of disease status. Since small changes in clone size and dynamics may influence clinical evaluation and decisions, the use of cfDNA for CHIP detection requires robust sequencing coverage and validation of variants at VAF<12%
Young:Novartis: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal